
Author: Aryan Kenia
Life Sciences Analyst
Retinol is one of the most proven skincare ingredients for improving skin texture, reducing fine lines, and evening skin tone. Modern delivery systems and better dose selection mean today’s retinol products can deliver visible results while minimising irritation.
A clinical study comparing 0.3% and 0.5% retinol serums showed that both concentrations improved hydration, pigmentation, and wrinkle depth. Importantly, 0.3% retinol delivered similar long-term benefits with fewer side effects, making it a strong option for consistent nightly use.
What are retinoids and why do they matter for skin?
Retinoids are a family of vitamin A derivatives used in skincare and dermatology. They work by binding to retinoic acid receptors in skin cells, triggering changes in gene expression that increase cell turnover, stimulate collagen production, and regulate pigmentation.
Prescription retinoids such as tretinoin are considered the gold standard for anti-ageing, but over-the-counter retinol and newer cosmetic retinoid derivatives can still deliver meaningful improvements when used correctly and consistently.

How to use retinol safely
- Start slow. Begin with application every third night and increase frequency gradually over 4 to 8 weeks.
- Use at night only. Retinoids increase sun sensitivity. Always apply sunscreen during the day.
- Support the skin barrier. Use a moisturiser rich in ceramides or lipids to reduce dryness and peeling.
- Avoid stacking strong actives. Do not use retinol at the same time as strong exfoliating acids until your skin has adapted.
- Pregnancy caution. Topical retinoids are generally not recommended during pregnancy. Consult a healthcare professional.
Retinol Evening Routine
Key clinical evidence: 0.3% vs 0.5% retinol
The table below summarises the main outcomes from the split-face, randomised 12-week study presented in your slides. Measurements were taken using validated instruments including Corneometer, Mexameter, PRIMOS 3D, and dermatologist scoring.
Clinical outcomes summary
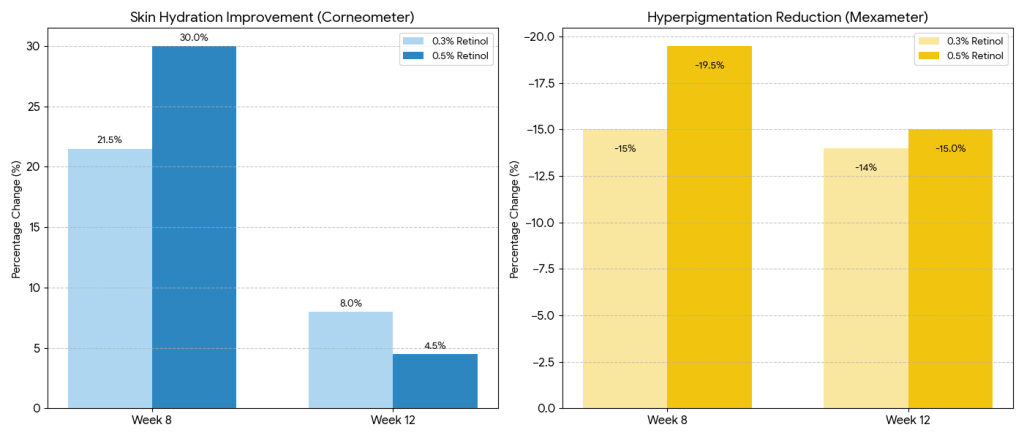
Skin hydration (Corneometer, cheek)
- Week 8:
- 0.3% retinol: +21.5%
- 0.5% retinol: +30%
- Week 12:
- 0.3% retinol: +8%
- 0.5% retinol: +4.5%
Interpretation: 0.5% produced a larger early hydration boost, but 0.3% retained hydration better over time.
Hyperpigmentation (Mexameter, cheek)
- Week 8:
- 0.3%: −15%
- 0.5%: −19.5%
- Week 12:
- 0.3%: −14%
- 0.5%: −15%
Interpretation: Both concentrations produced meaningful pigment reduction, converging by week 12.
Redness / erythema (Mexameter)
- Week 12 reductions ranged from 6% to 11.5% depending on site and concentration.
Interpretation: Redness decreased modestly, indicating the formulas were generally well tolerated on average.
Wrinkle depth (PRIMOS 3D)
- Average maximum wrinkle depth reductions ranged from approximately 40 to 108 micrometres after 12 weeks for both concentrations.
Subjective tolerability
- 0.3% retinol: High satisfaction with fewer reports of peeling, burning, and tightness.
- 0.5% retinol: Similar satisfaction but significantly more irritation, especially around week 8.
Overall conclusion:
0.3% retinol offers a better benefit-to-tolerability balance for long-term nightly use.
Retinoid types and how they differ
Consumer-friendly overview
- Retinol: Improves texture and fine lines with gradual use. Suitable for most users.
- Retinaldehyde: Stronger than retinol and closer to prescription strength.
- Hydroxypinacolone retinoate (HPR): A modern cosmetic retinoid with good stability and lower irritation in some studies.
- Prescription retinoids (tretinoin, adapalene): Highest efficacy but higher irritation risk.
- Bakuchiol: A non-retinoid alternative for those unable to tolerate vitamin A derivatives.
| Retinoid | What to expect | Relative strength | Best for |
|---|---|---|---|
| Retinyl esters (e.g., retinyl palmitate) | Gentle, slow acting; useful for maintenance | Low | Very sensitive skin, daily maintenance, formulations prioritising stability |
| Retinol | Gradual improvement in texture, pore appearance and fine lines | Moderate | First-time retinol users, general anti-ageing |
| Retinaldehyde | Faster results than retinol with somewhat higher activity | High | Users wanting stronger renewal with manageable irritation |
| Hydroxypinacolone retinoate (HPR) | Retinoid-like benefits with generally lower irritation in studies | Moderate to high | Cosmeceutical lines, consumers seeking potent but tolerable options |
| Tretinoin (prescription) | Strongest anti-ageing and acne activity, can be irritating | Very high | Medical treatments for photoageing and acne under clinician supervision |
| Adapalene (OTC/Rx) | Effective, stable, good tolerability for acne and some texture benefits | High for acne | Acne-focused products and tolerant skin types |
| Tazarotene (prescription) | Very potent, often more irritating than tretinoin | Very high | Strong clinical interventions for photoageing and psoriasis under supervision |
| Bakuchiol (plant-based alternative) | Retinol-like visual effects reported with lower irritation for some users | Low to moderate | Sensitive skin, pregnancy alternatives after medical advice |
Technical comparison for consultants and R&D teams
Retinyl esters (e.g. retinyl palmitate)
- Require multiple conversion steps to become active.
- Low potency but high stability.
- Useful for sensitive skin or maintenance products.
Retinol
- Converts in skin to retinaldehyde and then retinoic acid.
- Moderate potency with strong evidence.
- Stability improved through encapsulation and oil-phase delivery.
- Typical cosmetic range: 0.01% to 1%.
- Clinical data supports 0.3% to 0.5% as effective ranges.
Retinaldehyde
- One conversion step from retinoic acid.
- Higher potency than retinol.
- Increasingly used in clinical-grade cosmetics.
Hydroxypinacolone retinoate (HPR)
- Directly binds retinoic acid receptors.
- High stability and promising tolerability.
- Independent long-term data still emerging.
Prescription retinoids
- Direct receptor agonists.
- Highest efficacy and irritation risk.
- Require medical supervision.
| Retinoid | Mechanism / activation | Stability profile | Typical cosmetic concentrations | Formulation notes and best practices |
|---|---|---|---|---|
| Retinyl esters (retinyl palmitate, retinyl acetate) | Require enzymatic conversion to retinol then retinaldehyde and retinoic acid | High stability in formulations | 0.01 – 1% | Good for sensitive lines, stable in emulsions; acts as reservoir but slower onset |
| Retinol | Converted in-skin to retinaldehyde then retinoic acid | Moderate stability; sensitive to oxidation | 0.01 – 1% (commonly 0.1 – 0.5% in consumer products) | Prefer oil-phase or low-water vehicles, encapsulation or beadlets improves stability and tolerance; include antioxidants and opaque packaging |
| Retinaldehyde | One enzymatic step to retinoic acid (faster conversion) | Moderate stability; more stable than retinoic acid but less stable than some esters | 0.025 – 0.1% (typical 0.05 – 0.1%) | Useful in mid-level products; advantages for pigmentation and wound repair endpoints; handle as more potent active in safety testing |
| Hydroxypinacolone retinoate (HPR) | Binds retinoic acid receptors directly without conversion | High stability relative to retinol | 0.01 – 0.3% | Very stable in formulations; often marketed for low irritation; validate with finished product clinicals as independent data is expanding |
| Tretinoin (all-trans retinoic acid) | Direct retinoic acid receptor agonist (no conversion needed) | Low stability in some vehicles; sensitive to formulation and packaging | Prescription strengths vary (e.g., 0.025 – 0.1% as Rx) | Requires medical supervision; potent clinical efficacy for ageing and acne; formulation must control irritation and phototoxicity |
| Adapalene | Selective RAR agonist with stabilised chemical structure | High stability; chemically robust | 0.1% (OTC) and 0.3% (Rx) | Good stability simplifies formulation; excellent acne evidence; less irritation than tretinoin for many patients |
| Tazarotene | Prodrug converted to active retinoid with high receptor potency | Moderate stability; potent and often irritating | Prescription dosing typically 0.05 – 0.1% | High potency for clinical applications; requires careful dosing and patient counselling |
| Bakuchiol | Non-retinoid botanical that modulates some similar pathways | Good stability | 0.5 – 1% commonly used | Use as alternative for sensitive users or those avoiding vitamin A; evidence shows retinol-like visual improvements in some trials but mechanisms differ |
Formulation and delivery considerations
The presentation highlights the importance of delivery systems such as liquid crystal serums, encapsulation, beadlets, and lipid nanocarriers.
Key formulation principles:
- Minimise oxygen and light exposure during manufacture.
- Use opaque, airless packaging with low headspace.
- Consider encapsulated retinol to reduce irritation and improve stability.
- Validate retinol assay and oxidation during accelerated and real-time stability testing.
Claim language and compliance
Use conservative, evidence-aligned claims unless supported by finished-product clinical trials.
Examples of compliant claims:
- “Helps reduce the appearance of fine lines and improve skin texture with regular use.”
- “Supports skin renewal when used as part of a nightly routine.”
Avoid implying medical treatment unless supported by prescription-level data.
Consultant checklist for product development
- Define target user tolerance and frequency of use.
- Select retinoid type and concentration accordingly.
- Design the vehicle for controlled release and barrier support.
- Choose packaging that limits oxygen and light exposure.
- Run an 8–12 week vehicle-controlled clinical study to support claims.
- Include clear consumer usage instructions to minimise irritation.
Bottom line for consumers
Retinol is a proven ingredient for smoother, clearer, and more even-looking skin. Using the right concentration in a well-formulated product and introducing it gradually delivers the best results with the least irritation. Based on clinical evidence, 0.3% retinol is a strong choice for long-term nightly use.
References
- Zasada et al. Clinical comparison of 0.3% vs 0.5% retinol serums.
- Mukherjee et al. Retinoids in the treatment of skin ageing.
- Motamedi et al. Clinician’s guide to topical retinoids.
- Diridollou et al. Clinical efficacy of retinaldehyde in skin ageing.

Leave a comment